Progression-Free Survival
For first-line treatment of adult patients with locally advanced or metastatic EGFR+ NSCLC
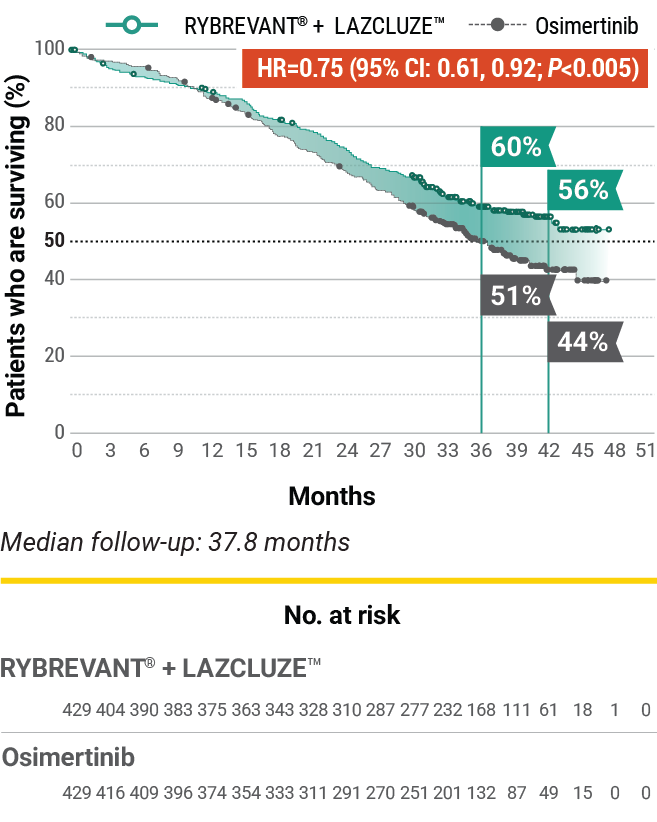
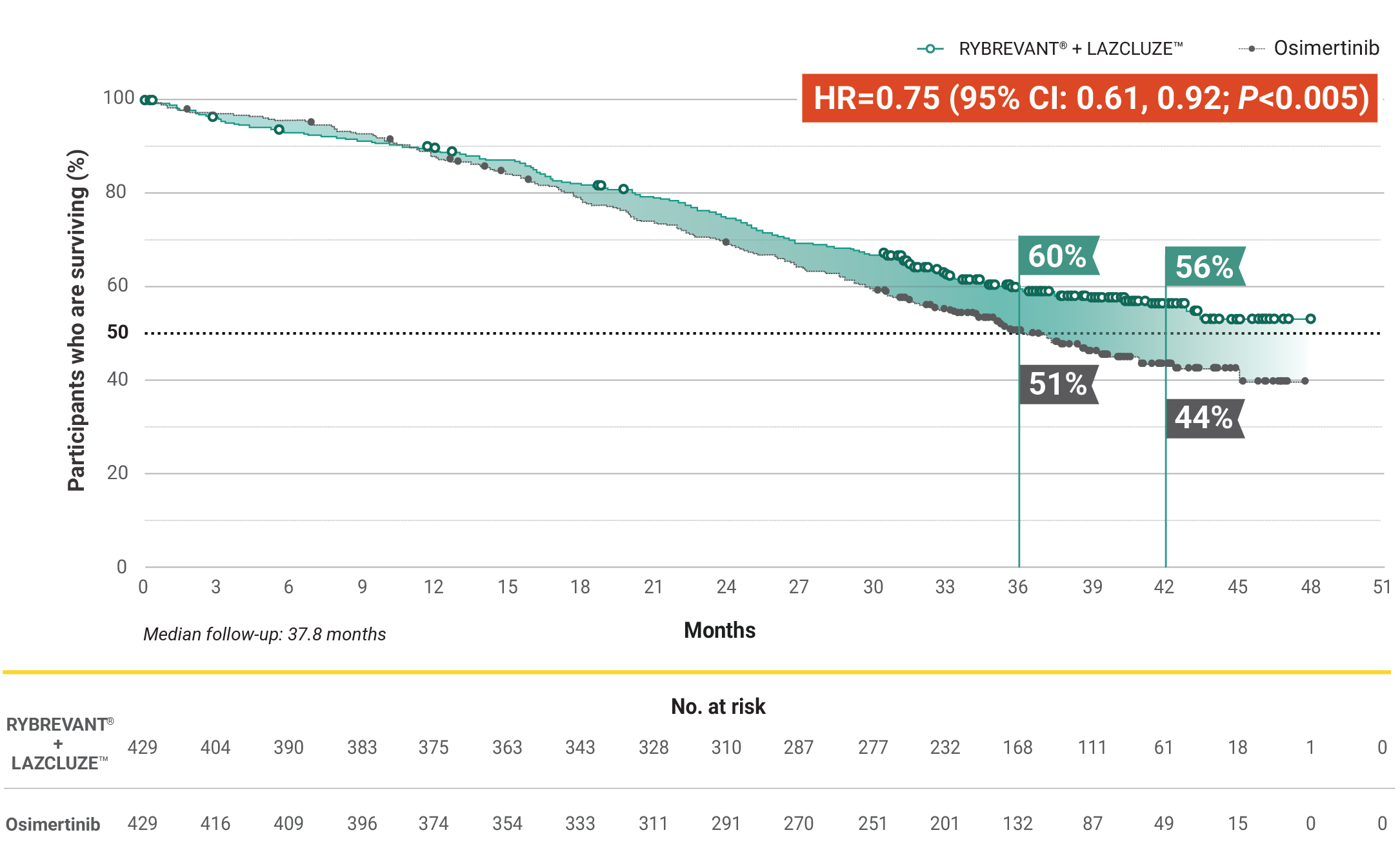
Superior PFS vs osimertinib with a chemotherapy-free combination1
RYBREVANT® + LAZCLUZE™ demonstrated a statistically significant reduction in the risk of progression or death by 30% vs osimertinib1,2
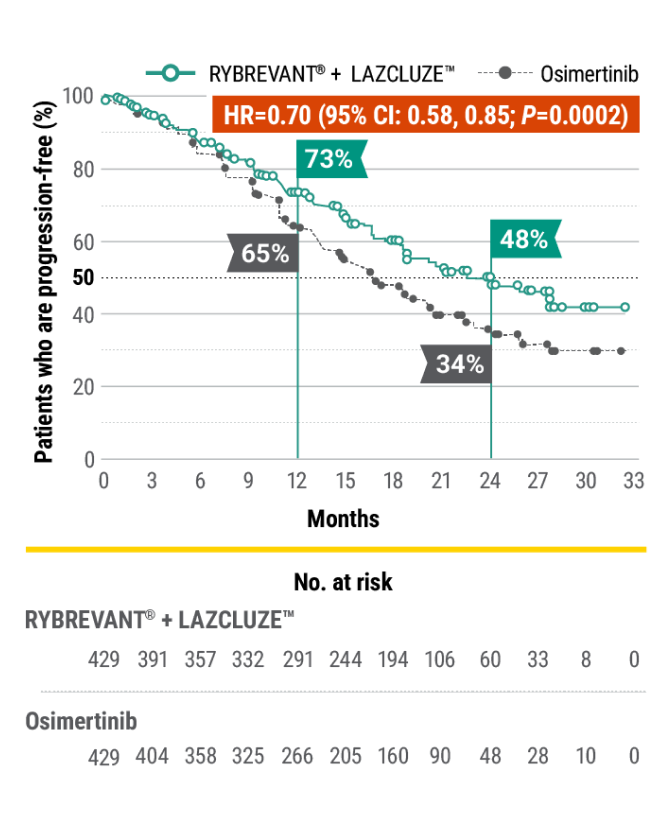
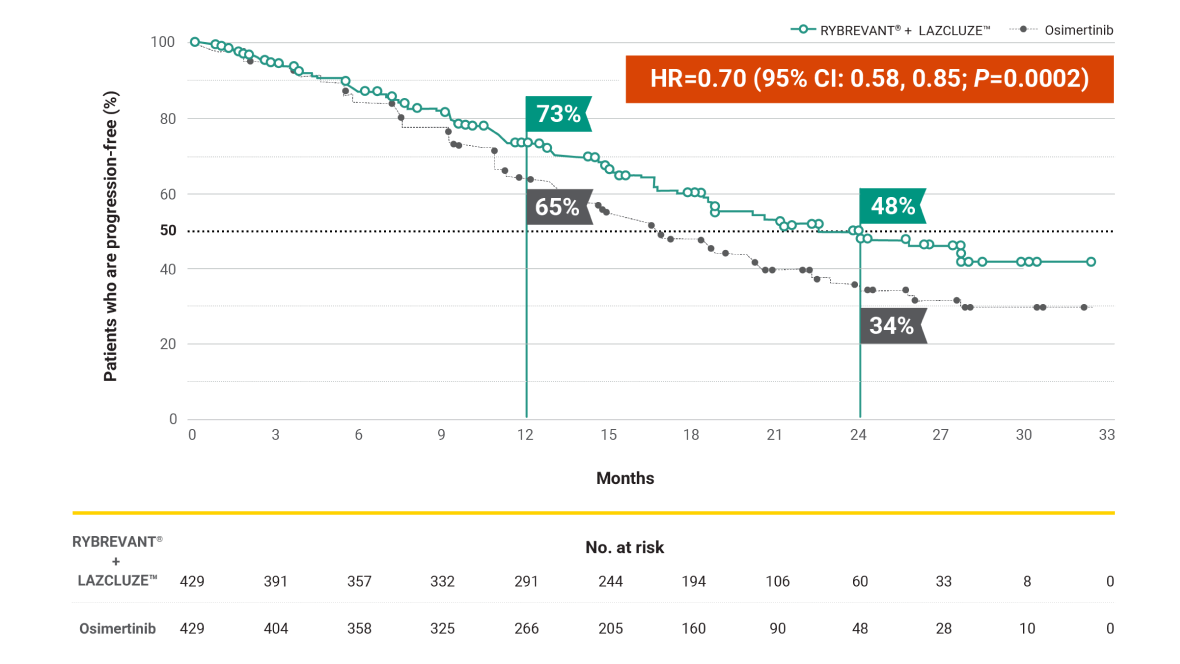
7.1-month improvement in mPFS vs osimertinib1
- 23.7 months (95% CI: 19.1, 27.7) mPFS with RYBREVANT® + LAZCLUZE™ vs 16.6 months (95% CI: 14.8, 18.5) with osimertinib
- In the non-registrational LAZCLUZE™ arm, median PFS was 18.5 months (95% CI: 14.8, 20.1)2
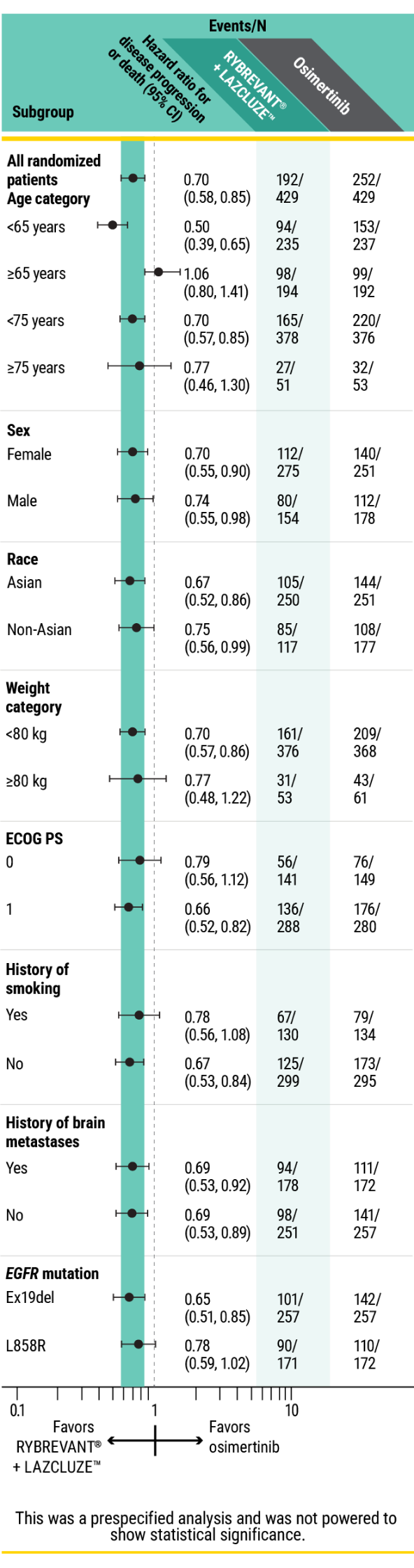
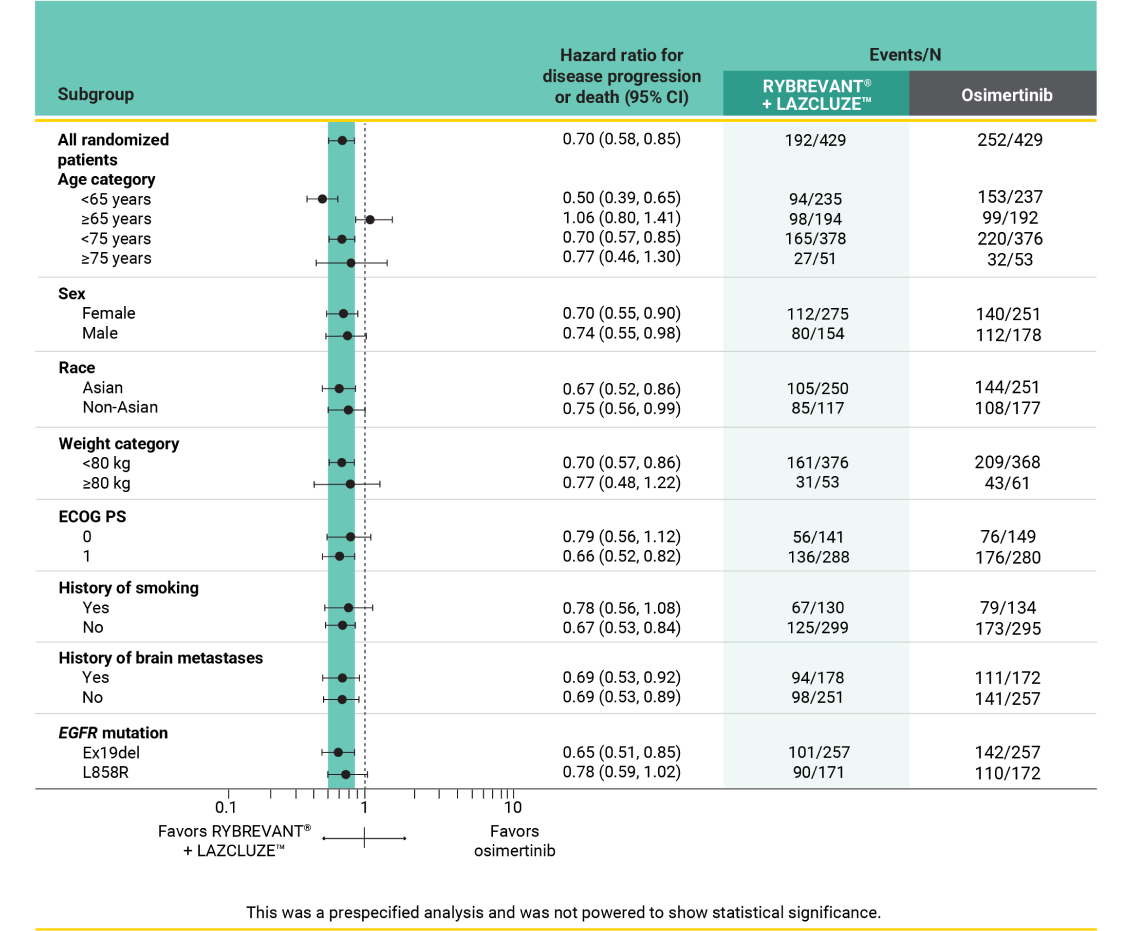
PFS results in prespecified subgroups2
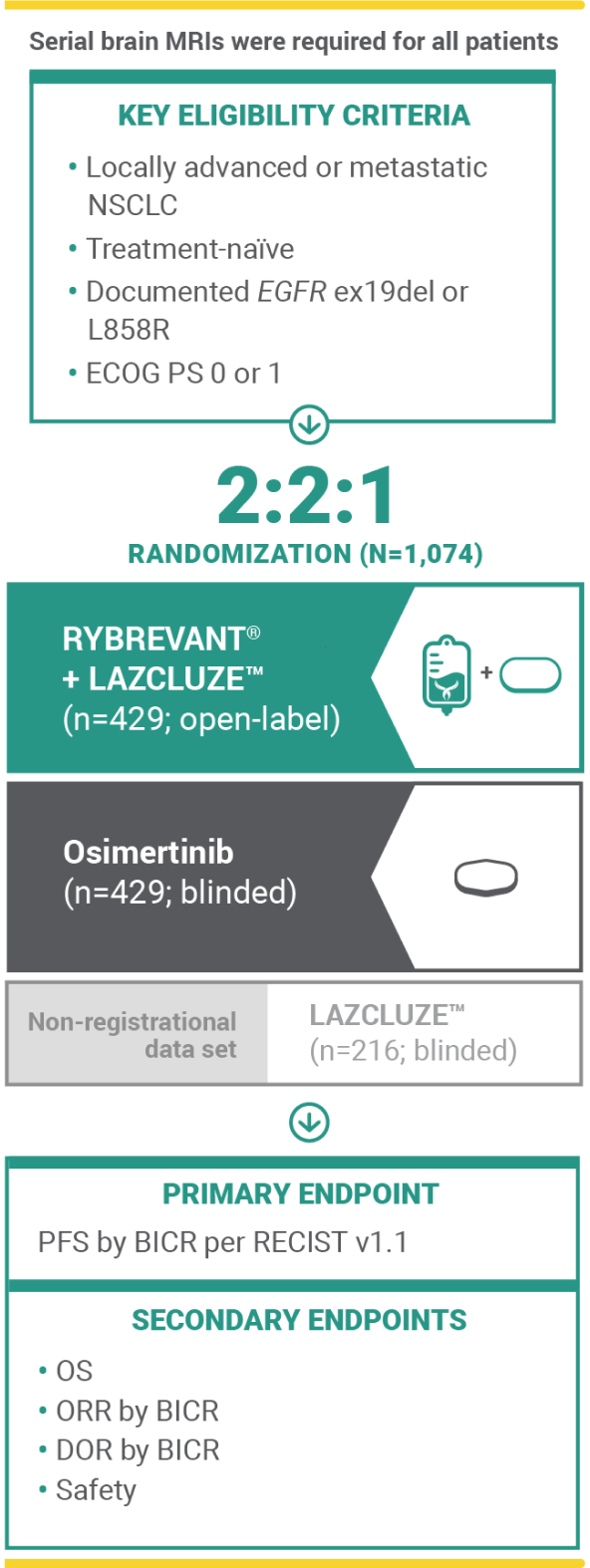
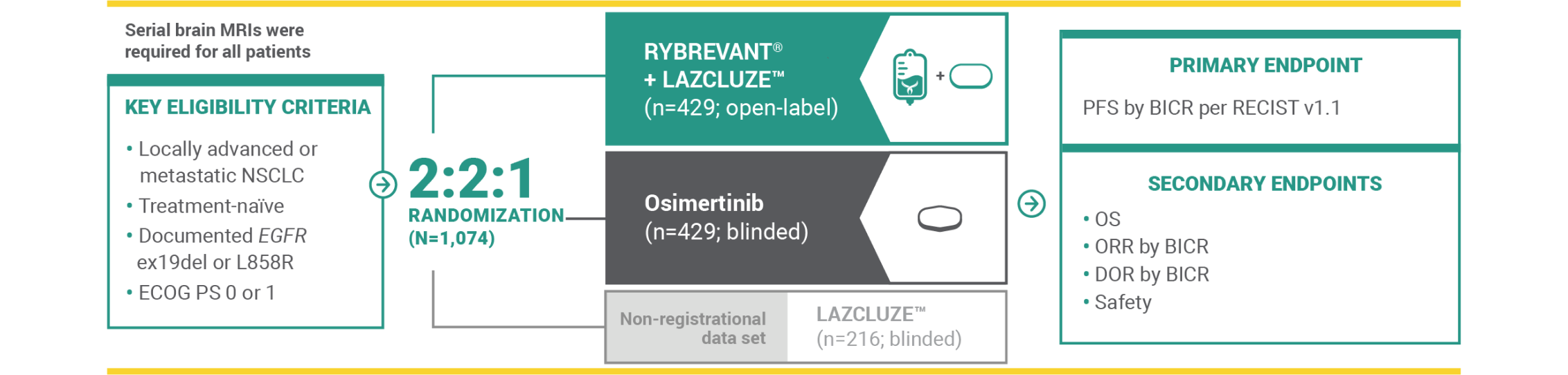
Methodology
In MARIPOSA, pathogenic alterations were identified using ctDNA by NGS of blood with Guardant360 CDx at baseline. Ex19del and L858R ctDNA in blood was analyzed at baseline with Biodesix ddPCR. This exploratory analysis included all randomized patients who had one or more biomarker assessment. Subgroup analyses of efficacy endpoints were carried out using statistical methods for the primary analysis of the general MARIPOSA population.3
Results
High-risk features at baseline, including detectable ctDNA, TP53 co-mutations, or metastases in the liver or brain, were identified in 89% of patients with baseline ctDNA available for NGS of pathogenic alterations (n=636).2,3

in risk of progression or death in patients with TP53 co-mutations treated with RYBREVANT® + LAZCLUZE™ (n=149) vs osimertinib (n=144) (HR=0.65 [95% CI: 0.48, 0.87])3
- mPFS of RYBREVANT® + LAZCLUZE™ was 18.2 months (95% CI: 15.3, 22.1) and 12.9 months (95% CI: 11.1, 14.7) with osimertinib

in risk of progression or death in patients with detectable ctDNA at baseline by ddPCR* with RYBREVANT® + LAZCLUZE™ (n=231) vs osimertinib (n=240) (HR=0.68 [95% CI: 0.53, 0.86])3
- mPFS of RYBREVANT® + LAZCLUZE™ was 20.3 months (95% CI: 16.6, 24.0) and 14.8 months (95% CI: 12.9, 16.5) with osimertinib

in risk of progression or death in patients with liver metastases at baseline treated with RYBREVANT® + LAZCLUZE™ (n=64) vs osimertinib (n=72) (HR=0.58 [95% Cl: 0.37, 0.91])3
- mPFS of RYBREVANT® + LAZCLUZE™ was 18.2 months (95% CI: 13.1, NE) and 11 months (95% CI: 7.4, 12.8) with osimertinib
This analysis is not included in the Prescribing Information for RYBREVANT® and LAZCLUZE™. This was a post hoc exploratory analysis and was not powered to show statistical significance.
*Consistent results were seen in patients with detectable ctDNA using the NGS assay (HR=0.71 [95% CI: 0.57, 0.89]).
CI, confidence interval; ctDNA, circulating tumor DNA; ddPCR, droplet digital polymerase chain reaction; DNA, deoxyribonucleic acid; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor; ex19del, exon 19 deletion; HR, hazard ratio; mPFS, median progression-free survival; NE, not estimable; NGS, next-generation sequencing; NSCLC, non–small cell lung cancer; PFS, progression-free survival.